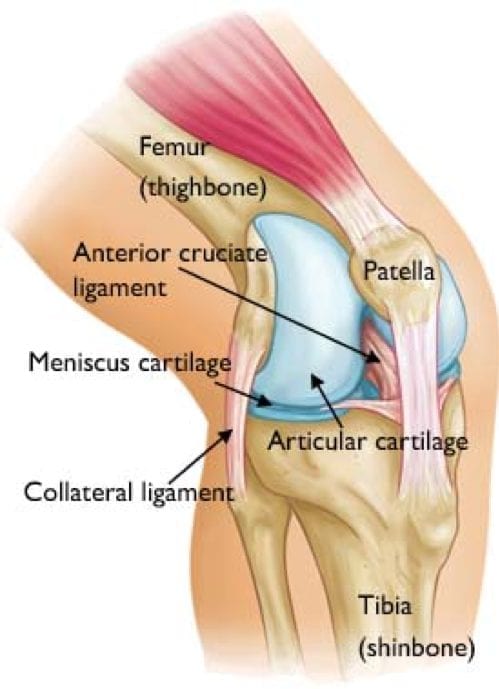
Knee problems can be complicated, but one basic concept will simplify your understanding of knee pain: that the knee pain is either internal (issues within the knee joint itself), or external (problems of the patellar quadriceps mechanism). Take a look at this picture of the knee so you’ll know what I’m talking about.
The Most Common Cause of Knee Pain
The knee joint itself is where motion occurs between the thigh bone (the femur) and the shin bone (the tibia).
But overlying the knee joint is the quadriceps muscle (not shown in this picture) along with the patella (kneecap) and the tendons attached to the patella (the patellar and quadriceps tendons). Problems with these patellar and quadriceps structures are the most common cause of knee pain.
Diagnostic possibilities within this general category include:
- Quadriceps tendinitis
- Patellar tendinitis
- Quadriceps strain
- Patellar maltracking
Are you interested in becoming a certified acupuncture professional?
Visit the links below to explore our specialized acupuncture programs at a campus near you:
Second Most Common Cause of Knee Pain
The next most common cause of knee pain is disruption of the ligaments or cartilage inside the knee joint. Some of the various problems inside the knee joint include injuries to the anterior cruciate ligament, the posterior cruciate ligament, or one of the menisci.
The good news is that most knee conditions can be treated with the right combination of acupuncture, body work, and rehabilitative exercises.
Western Approach to Knee Pain Treatment
Testing Western
As part of the acupuncture curriculum, we each learn several orthopedic assessment exams. These exams are great at diagnosing issues involving the knee joint: the Anterior Drawer Test, for ACLs; the Varus Stress Test, for LCLs; the Valgus Stress Test, for MCL; and others that also include testing for possible meniscus tears, like the McMurry’s Test, and the Bounced Home Test.
The only problem with these orthopedic assessment exams is that they only cover the second most common cause of knee pain. They are not helpful in diagnosing issues involving individual muscles or muscle groups.
Manual muscle testing is a great way to assess issues involving the quadriceps muscles, which are usually involved in the most common cases of knee pain. The muscles of the quadriceps are first tested as a group, then rectus femoris, vastus lateralis, and vastus medialis are tested individually.
When testing a muscle, it is given a grade from 5 to 0.
Grade 5 (Normal)
The patient or subject can complete the whole range of motion (movement) against gravity with maximum resistance applied at end of range.
Grade 4 (Good)
The subject can complete the whole range of motion against gravity with moderate resistance applied at end range.
Grade 3 (Fair)
The patient can only complete the range of motion against gravity. When external (outside) force is applied, the patient gives way.
Grade 2 (Poor)
The patient cannot perform the movement against gravity, but can do complete range of motion when pull of gravity is eliminated. No resistance is applied.
Grade 1 (Trace)
Patient is not able to move the joint even with gravity eliminated. However, slight muscle contraction can be felt through palpation.
Grade 0 (No trace)
No contraction is noticed, even with palpation.
Eastern Approach to Knee Pain Treatment
Treating Eastern
Once the hypertonic (tight muscle), has been identified, the practitioner can begin to formulate a treatment plan. I have found local needling (in the affected muscle) combined with distal needle placement to be the most beneficial approach in treating knee pain.
Most acupuncturists, while in school, become familiar with a knee treatment protocol called “the seven needle knee”. This local needling treatment involves placing seven needles in specific points: ST34, Heding, SP10, ST35, Xiyan, SP9, and ST36.
In my practice, I’ve modified this treatment protocol to one that I have found to be extremely effective in treating both external, and internal knee pain conditions:
- ST34 is replaced with the extra point Xinfutu. It is located 1-2 cun lateral from ST32. I use this point to reset vastus lateralis.
- Heding is replaced with needling the midpoint between Heding and ST31. This location is used to reset rectus femoris.
- SP10 is replaced with the extra point Baichongwo. Vastus medialis can be reset needling this point.
- ST35, Xiyan, and SP9 remain the same, except that SP9 is needled in an upward direction until the needle touches the bone. This is done to stimulate the periosteum surrounding the tibia (the membrane that covers the outer surface of all bones).
- ST36 is replaced with Master Tung point 77.08. 77.08’s location is very similar to ST36, except that it is needled as high and close to the tibia as possible.
Distal needle choices depend on the acupuncturist system of choice. Each system, or combination of systems, seems to work well with the above approach. Since vastus lateralis and rectus femoris are related to the stomach or foot yang ming, while vastus medialis is related to spleen or foot tai yin, the selection of distal points should correlate with and treat these pathways.
Featured Posts:
